Where we die now…
• Jeremy Faust writes in his Substack Inside Medicine blog about how more and more Americans are choosing to die at home; it’s worth a read. Some numbers from his post:
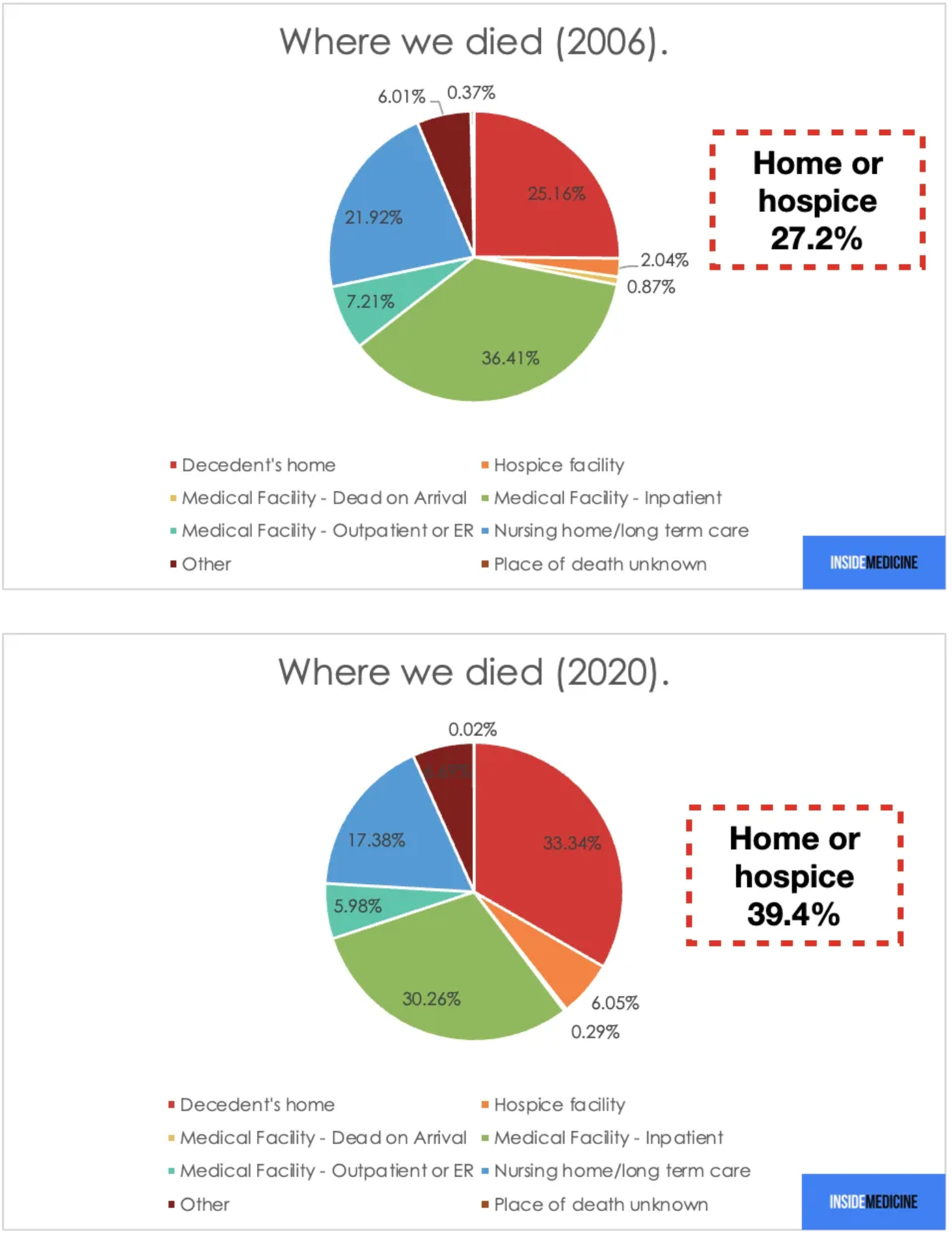

• Jeremy Faust writes in his Substack Inside Medicine blog about how more and more Americans are choosing to die at home; it’s worth a read. Some numbers from his post:
• Jeremy Peters and Katie Robertson write in the NY Times about some of the noisome evidence produced in the Dominion defamation case. For me, the most heinous indictment in their story comes in this quote from Rupert Murdoch:
“On one occasion, as Mr. Murdoch watched Mr. Giuliani and Ms. Powell on television, he told Suzanne Scott, chief executive of Fox News Media, “Terrible stuff damaging everybody, I fear.””
Murdoch knew the damage he was doing to people and to this country and yet persisted, all in the interest of $$. Read the story, it says it all about the profit driven business plan of his media empire, one built on lies and fear-stoking.
I enjoyed this interview with Steven Pinker on ChatGPT in the Harvard Gazette. From the piece:
“It’s impressive how ChatGPT can generate plausible prose, relevant and well-structured, without any understanding of the world — without overt goals, explicitly represented facts, or the other things we might have thought were necessary to generate intelligent-sounding prose.
And this appearance of competence makes its blunders all the more striking.”
Some data on excess death rates among physicians before and after the availability of Covid vaccines. From JAMA Internal Medicine: Kiang MV, Carlasare LE, Thadaney Israni S, Norcini JJ, Zaman JAB, Bibbins-Domingo K. Excess Mortality Among US Physicians During the COVID-19 Pandemic. JAMA Intern Med. Published online February 06, 2023.
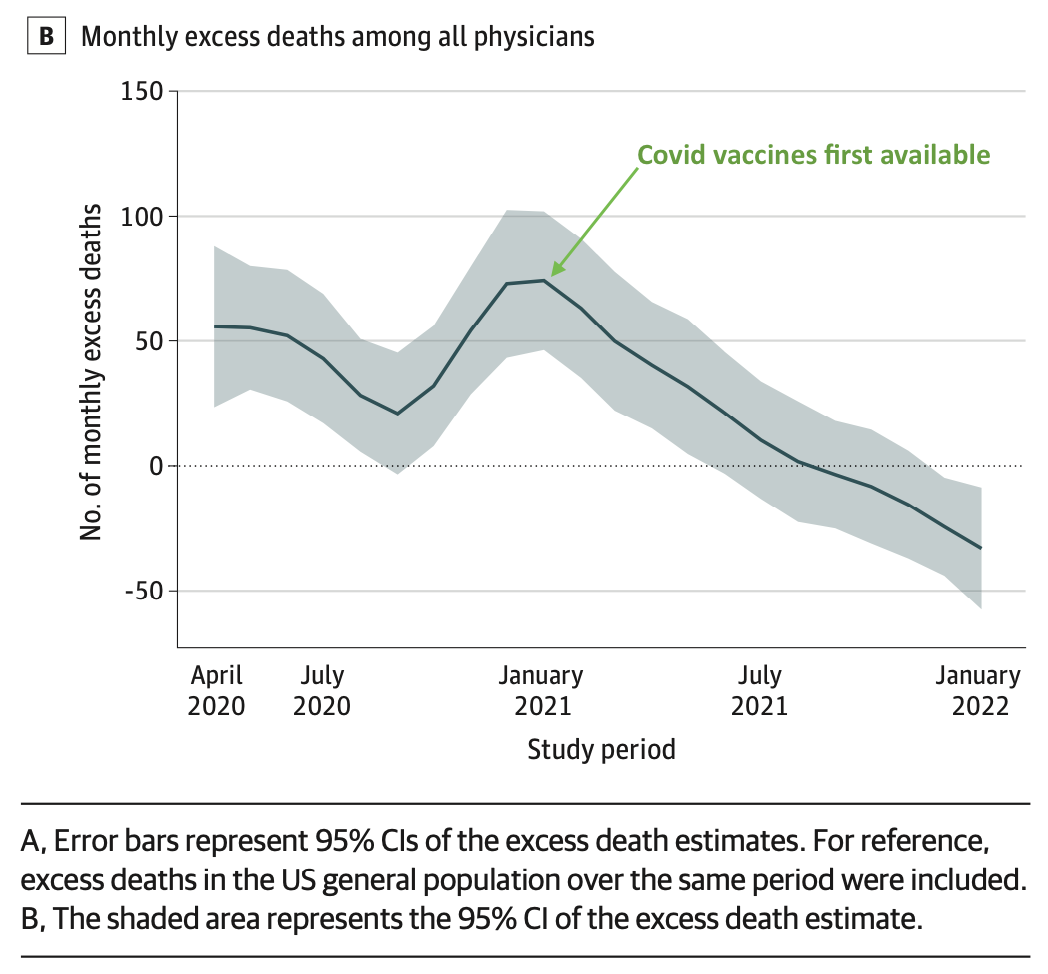
“From March 2020 through December 2021, US physicians experienced 622 more deaths than expected. There were no excess deaths among physicians after April 2021, coinciding with the widespread availability of COVID-19 vaccines.”
• Dr F. Perry Wilson of the Yale School of Medicine writes on Medscape about this interesting article from Plos One: “U.S. state policy contexts and mortality of working-age adults” by Montez, Mohri, Monnat, et al. Dr. Wilson thinks that average education level may be the primary factor for the life expectancy discrepancy between states rather than state policies, but the authors in their abstract suggest that state policies may have a large impact:
“Simulations indicate that changing all policy domains in all states to a fully liberal orientation might have saved 171,030 lives in 2019, while changing them to a fully conservative orientation might have cost 217,635 lives.”
and in their discussion:
“On average, Americans die younger than their peers in most other high-income countries. In a 2013 U.S. survey, 85% of adult respondents indicated that their ideal life span was 79 years or older, yet U.S. life tables predicted that only 60% of people born that year could expect to survive to age 79 [40, 41]. Our findings, which examine working-age deaths among adults ages 25–64 years, suggest state policies–specifically, their left/right lean–may be a contributing factor and provide new insights into potential strategies to reduce working-age mortality.”
The always-wonderful Eric Foner writes in the NYT about using the 14th amendment’s Section 4 to avert a Republican-induced debt ceiling crisis:
“The validity of the public debt of the United States,” it declares, “shall not be questioned.”
No, medical error is NOT the third leading cause of death, and no, Emergency Department misdiagnoses are NOT killing 250,000 people a year in the U.S. As an emergency physician, the widely publicized AHRQ report is particularly painful because it has numerous flaws, and like the Institute of Medicine /BMJ study, is guilty of completely unwarranted extrapolations. The authors, for instance, looked at a Canadian study on 503 patients discharged from EDs, one of who died within 14 days of the ED visit (it’s not clear whether this actually represented a diagnostic error; the study was looking at outcomes after the visit, not misdiagnoses). The AHRQ study then took this single death from a single study to establish a 0.2% (1/503) death rate due to ED diagnosis and multiplied it by the 130 million total annual ED visits to get the purported death numbers. They went on to concoct arbitrary confidence intervals for this extrapolation:
“The rate of misdiagnosis-related deaths in the one high-quality, prospective study (0.2 percent, n=1 of 503) is 217-fold higher than the weighted mean from the three retrospective studies (0.0009 percent). Although the rate of 0.2 percent is based on just a single death (so is imprecise, with a wide 95% CI 0.005 to 1.1), the value is the best estimate from this study and matches data from other sources. However, the confidence interval from the Calder study alone is implausibly wide. Based on data from other sources, we have assigned a +/- 2-fold plausible range to the 0.2 percent estimate (0.1% to 0.4%).”
This is not good science. For more, see:
• An excellent podcast by Ezra Klein, interviewing Gary Marcus’ “Skeptical Take on the A.I. Revolution”; definitely worth a listen.
• Mihir Desai at HBS and HLS opines — correctly in my mind — about the illusory promises of the crypto kingdom in his opinion piece in the NYT.
Yet another sadly undistinguished rip off by Twitter as used office inventory goes out for auction…